

Is ICL Surgery Suitable for Asian Eyes? What Does the Research Show?
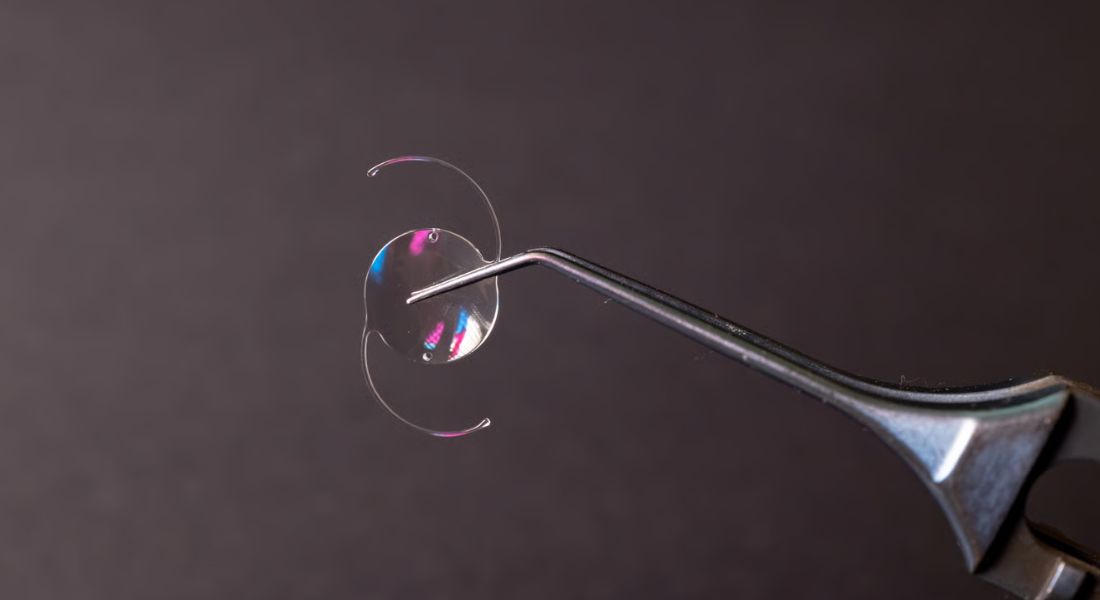
ICL surgery, also known as implantable collamer lens surgery, is a vision correction procedure where a thin specialist lens is placed inside your eye to correct refractive errors such as myopia and astigmatism. It is often considered when laser eye surgery may not be the most suitable option due to prescription strength, corneal thickness, or other eye health factors.
In Asian patients, ICL surgery is frequently discussed because myopia is more common in many Asian populations, and a higher proportion of patients may have moderate to high prescriptions. In some cases, these levels of myopia can make corneal laser surgery less suitable, which is why ICL may be considered as an alternative that preserves the corneal structure.
Research also shows that ICL planning depends heavily on detailed anatomical measurements of the eye. These include anterior chamber depth, white-to-white distance, lens position, and the expected postoperative vault. Careful assessment of these factors is essential to ensure the lens fits safely and performs well over time.
Overall, the research suggests that ICL surgery can be suitable for many Asian eyes when proper measurements and safety criteria are met. However, suitability is always based on individual eye anatomy and clinical findings, not ethnicity alone. Your personal scan results and eye health assessment are what ultimately determine whether ICL is appropriate for you.
What Is ICL Surgery?
ICL surgery involves placing a thin, implantable lens inside your eye to help correct vision problems such as myopia and astigmatism. Your natural lens is left in place, which is why this procedure is called a phakic intraocular lens surgery. It is designed to improve vision while preserving the eye’s natural focusing structures.
The ICL is usually positioned behind your iris and in front of your natural lens. Once in place, it works together with your eye’s existing optical system to help light focus more accurately on the retina, resulting in clearer and sharper vision. The procedure is carefully planned to ensure the lens fits safely within your eye.
Unlike LASIK, ICL surgery does not involve reshaping, thinning, or removing any corneal tissue. Instead, it corrects vision from inside the eye while maintaining the natural structure and strength of your cornea, which can be an important advantage for certain patients.
Why ICL Is Often Discussed for Asian Patients
ICL is often discussed for Asian patients because myopia, including high myopia, is more common in many Asian communities. In these cases, laser vision correction is not always the safest or most suitable option, depending on the individual’s eye anatomy and prescription level.
If your prescription is high, LASIK may require a greater amount of corneal tissue removal to achieve the desired correction. If your cornea is thin or borderline in thickness, ICL may be considered instead because it corrects vision inside the eye without reshaping the corneal surface.
Research in Asian populations has generally shown good visual outcomes after ICL implantation for high myopia. One study of ICL V4c implantation reported good efficacy, safety, predictability, and stability over a 12-month follow-up period. These results support ICL as an effective option when patients are carefully selected and properly assessed.
Asian Eyes Are Not All the Same
The phrase “Asian eyes” is very broad and can include East Asian, South Asian, Southeast Asian, West Asian, and mixed-heritage patients. These groups are often discussed together in research, but in reality, there can be significant variation between individuals.
Eye anatomy can differ quite a lot even within the same ethnic group. For example, two Asian patients with the same prescription may still have very different anterior chamber depth, corneal thickness, white-to-white measurements, and overall internal eye structure. These differences can directly affect ICL planning and suitability.
This is why ICL suitability should never be based on ethnicity alone. Your individual scans and measurements are far more important, as they provide a clear and accurate picture of whether the procedure is safe and appropriate for your specific eyes.
The Role of High Myopia
High myopia (a strong short-sighted prescription) is one of the main reasons you might be considered for ICL surgery. When prescriptions are very high, laser eye surgery may not always be suitable because there may not be enough corneal thickness left after treatment. In these situations, ICL can be a useful alternative because it corrects vision without removing corneal tissue.
- Why ICL Is Considered: If you have high myopia, laser procedures like LASIK, PRK, or SMILE may be limited by how much corneal tissue would need to be removed.
- Tissue-Sparing Approach: ICL corrects your vision by placing a lens inside the eye, so your cornea is left untouched.
- Useful for Strong Prescriptions: It can be especially helpful if your prescription is too high for safe or effective laser correction.
- Retinal Health Needs Attention: With high myopia, you may have a higher risk of retinal thinning or tears, so a detailed examination of the back of your eye is essential before surgery.
- Careful Pre-Operative Assessment: Your surgeon will check your retina and overall eye health to make sure ICL is safe and appropriate for you.
Overall, high myopia is often a key factor when considering ICL surgery, but it also means your eyes need a thorough assessment before any procedure. While ICL can be a very effective option, careful screening of your retina is essential to ensure long-term safety and the best possible outcome.
Suitability Depends on Eye Anatomy
ICL suitability depends mainly on the internal structure of your eye. Your surgeon needs to carefully assess whether there is enough safe internal space for the lens to sit comfortably and securely without affecting the natural structures of your eye or disrupting normal fluid flow. This is a key safety step in determining whether the procedure is appropriate for you.
Key measurements include anterior chamber depth, white-to-white distance, sulcus anatomy, lens rise, eye pressure, endothelial cell count, and overall eye health. Current ICL guidance also refers to minimum anatomical requirements, including sufficient anterior chamber depth and appropriate white-to-white measurements, to ensure the lens can be safely implanted.
This means that even if your prescription is suitable for ICL, you may still not be a candidate if your eye anatomy does not meet safety criteria. Careful measurement and assessment are therefore essential to ensure the procedure is both safe and effective for your individual eyes.
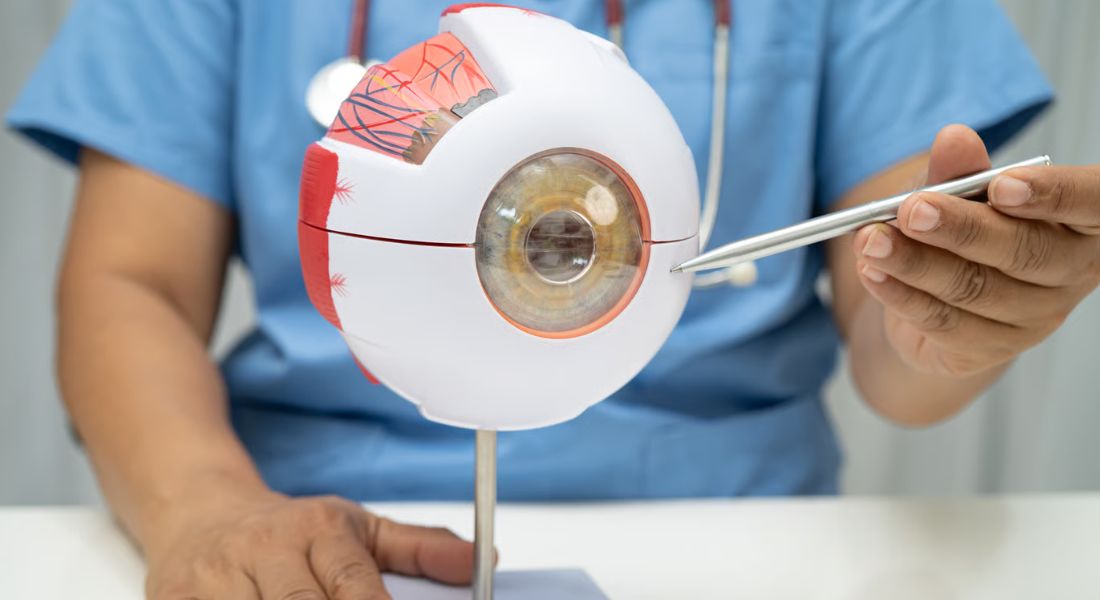
Anterior Chamber Depth
Anterior chamber depth is the space between the back of your cornea and the front surface of your natural lens. This measurement is very important because the ICL needs enough internal space to sit safely and comfortably inside your eye.
If your anterior chamber is too shallow, there may be a higher risk of crowding inside the eye or pressure-related issues. This does not automatically mean you cannot have ICL surgery, but it does mean your case needs very careful assessment and planning by a specialist.
A recent study found that ICL surgery in American eyes with anterior chamber depths below 3.0 mm could still produce good outcomes in selected patients. However, decisions like this are highly individual and must be based on detailed measurements, safety considerations, and expert clinical judgement.
White-to-White Measurement
White-to-white measurement refers to the horizontal visible diameter of your cornea, measured from one white edge of the eye to the other. It is commonly used as part of the planning process for ICL surgery to help estimate the size of the lens that may be suitable for your eye.
However, white-to-white measurement alone does not fully reflect the internal space where the ICL will actually sit. Because of this limitation, many surgeons also rely on additional imaging techniques and more advanced calculation formulas to get a more accurate understanding of your eye’s internal anatomy.
In Asian patients in particular, precise sizing is very important, as even small anatomical differences can affect postoperative vault and overall lens positioning. This is why detailed measurements and careful surgical planning are essential for achieving safe and predictable outcomes.
What Is Vault?
Vault is the space between the back surface of the ICL and the front surface of your natural lens inside the eye. It is one of the most important safety measurements used before and after ICL surgery because it helps determine how safely and comfortably the lens sits inside your eye over time.
If the vault is too low, the ICL may sit too close to your natural lens, which can increase the risk of contact-related issues over time. If the vault is too high, it may affect the drainage angle of the eye or influence eye pressure, which is why careful monitoring is essential.
Good ICL planning focuses on predicting a safe and appropriate vault before surgery and then monitoring it after the procedure. This helps ensure that the lens remains stable, safe, and well-positioned for long-term visual health.
Vault Prediction in Asian Eyes
Vault prediction is an important area of research in ICL surgery, as it helps determine how well the lens will sit inside your eye after implantation. A 2025 study comparing predicted and achieved postoperative vaults found that the NK-V3 formula performed better than NK-V2 in Asian eyes, while showing comparable results in White eyes.
This is significant because it suggests that some sizing formulas may perform differently depending on the population being studied. It also highlights why researchers continue to develop newer calculation methods and improve imaging techniques to make predictions more accurate and reliable.
For you as a patient, the key message is that ICL sizing should always be personalised. The best outcomes come from using detailed measurements of your eye rather than relying on a one-size-fits-all approach, ensuring the lens is selected safely and accurately for your individual anatomy.
ICL Sizing Formulas
ICL sizing formulas help your surgeon choose the most suitable lens size so that it sits safely inside your eye after surgery. The goal is to achieve an appropriate “vault”, which is the space between the implant and the natural lens. If the sizing is not accurate, it can affect safety and visual outcomes, so careful planning is essential.
- Purpose of Sizing Formulas: These formulas help predict how the ICL will fit inside your eye and support a safe postoperative vault.
- Evolving Measurement Methods: Older approaches used fewer eye measurements, while newer methods often include more detailed anatomical data.
- Multiple Valid Approaches: Research suggests that several different published formulas can produce good results when used correctly.
- Technology and Experience Matter: The best method often depends on the surgeon’s diagnostic tools, clinical experience, and planning systems.
- No Single Perfect Formula: There is no one-size-fits-all approach, so careful individual assessment is always required.
Overall, ICL sizing is not based on a single fixed calculation but on a combination of measurements and clinical judgement. Your surgeon will choose the most appropriate method based on your eye’s anatomy and the available imaging data. This personalised approach helps improve both safety and visual outcomes after surgery.
Artificial Intelligence and ICL Planning
Artificial intelligence is increasingly being explored in ICL planning, particularly for predicting vault and helping with lens sizing. AI can analyse multiple eye measurements at the same time and identify patterns that traditional calculation formulas may not always detect.
A study using big data and AI has aimed to predict EVO ICL vault and lens size, showing how machine learning could support more personalised surgical planning. These tools may help improve accuracy and reduce uncertainty in selecting the most suitable lens for each patient.
For you as a patient, especially if you are Asian, AI-based tools may be particularly relevant because many ICL datasets and vault prediction studies include a large number of Asian eyes. However, these tools are still supportive, and final decisions always rely on your surgeon’s clinical judgement and full eye assessment.
Machine Learning for Vault Prediction
Machine learning is becoming an increasingly important tool in ICL planning. It can analyse pre-operative eye measurements and help estimate postoperative vault more accurately, which is important for choosing the correct lens size.
A 2025 study reported that artificial intelligence can effectively predict postoperative vault and assist in determining ICL sizing, with the XGBoost model performing better than other tested machine-learning algorithms. These developments suggest that AI may improve the precision of surgical planning.
However, machine learning is not a replacement for clinical judgement. It should be used as a supportive tool to assist the surgeon, who will always make the final decision based on a full assessment of your eye health and anatomy.
ICL Outcomes in Asian Patients
Research in Asian patients has generally shown good visual outcomes when the procedure is performed in carefully selected candidates. The ICL V4c high myopia study reported favourable vision results and stable outcomes during follow-up, which supports its effectiveness in appropriate cases.
This is particularly encouraging if you have high myopia and are not an ideal candidate for laser eye surgery. In such situations, ICL can offer a strong alternative by improving vision while preserving the corneal structure.
However, your outcome is not only dependent on the lens itself. It also relies on correct patient selection, accurate sizing, surgical technique, and proper follow-up care. A successful result is not just about reducing your prescription, but also about maintaining long-term eye health and visual stability.
ICL for Low to Moderate Myopia
ICL surgery has traditionally been used most often for high myopia, but more recent research has also explored its use in low to moderate myopia. This is important because some patients may prefer ICL even when their prescription is not very high, especially if they are not suitable for laser vision correction.
A 2025 study noted that an increasing number of patients with low to moderate myopia are interested in ICL implantation. It also reported that some short-term outcomes in these patients can be comparable to those seen in individuals with higher levels of myopia, particularly in terms of visual quality and satisfaction.
However, ICL should not be chosen simply because it is available as an option. Your suitability still depends on detailed eye measurements, internal anatomy, safety factors, and your personal visual goals. A careful assessment is essential to ensure the procedure is appropriate for you.
ICL for Astigmatism
Many Asian patients with myopia may also have astigmatism. In suitable eyes, toric ICL lenses can correct both myopia and astigmatism at the same time, which can improve overall visual clarity and reduce dependence on glasses.
With toric ICL, accurate lens alignment is very important. If the lens rotates after surgery, the level of astigmatism correction may become less precise, which can affect visual quality. This is why stability and correct positioning are key parts of surgical planning.
Before recommending toric ICL, your surgeon will carefully assess your eye anatomy, expected lens positioning, and overall suitability. These measurements help ensure the lens remains stable and provides the most accurate and predictable visual outcome.
Thin Corneas and ICL
One reason you may be offered ICL surgery is if you have thin corneas. Because ICL does not involve removing corneal tissue or reshaping the surface of your eye, it can be a suitable option for some patients who are not ideal candidates for LASIK or other laser procedures.
This can be particularly relevant if you have high myopia, as laser correction may require more corneal tissue removal to achieve the desired result. In such cases, ICL may help preserve your natural corneal structure while correcting your vision from inside the eye.
However, having thin corneas on its own does not automatically mean you are suitable for ICL. Your internal eye measurements, such as anterior chamber depth and overall ocular anatomy, still need to meet strict safety requirements before the procedure can be recommended.
Dry Eye Considerations

Some patients consider ICL surgery because they already experience dry eye symptoms or have difficulty tolerating contact lenses. Since ICL does not involve creating a corneal flap or reshaping the surface of the eye like LASIK, it may be a more suitable option for selected patients with dry eye concerns.
However, dry eye still needs careful assessment before surgery. Even though the cornea is not reshaped, a healthy and stable ocular surface is still important for achieving clear, comfortable vision and good visual quality after any refractive procedure.
Your surgeon should therefore evaluate your symptoms, tear film quality, eyelid health, and any underlying allergy or inflammation. Addressing these factors beforehand can help improve comfort, reduce postoperative symptoms, and support better overall outcomes.
Eye Pressure and Angle Assessment
Because ICL is placed inside your eye, checking your eye pressure and drainage angle is an essential part of the assessment. Your surgeon needs to understand how fluid moves within your eye and whether the lens could affect this natural drainage system.
If your drainage angle is narrow or there are any concerns about eye pressure, ICL surgery may require extra caution, or in some cases it may not be recommended. Although modern ICL designs have improved safety and compatibility, careful screening is still essential before moving forward.
This assessment is particularly important if your eyes have smaller internal dimensions, as there may be less space for the lens and a higher need for precise planning to ensure safe and stable outcomes. In such cases, even small variations in measurement can influence safety decisions, so detailed imaging and careful interpretation of results are crucial to achieving the best possible long-term outcome for your vision.
Endothelial Cell Count
The corneal endothelium is the thin inner layer of cells that helps keep your cornea clear by controlling fluid balance. These cells are particularly important because they do not regenerate significantly, so maintaining a healthy count is essential for long-term corneal health.
Before ICL surgery, your surgeon will usually measure your endothelial cell count. This test helps confirm that your cornea has enough healthy cells to safely support an intraocular lens procedure. It is a key part of ensuring the surgery is appropriate for your eyes.
After surgery, long-term follow-up may also include periodic endothelial monitoring. This is especially important if there are any concerns, as it helps ensure your cornea remains healthy and continues to function properly over time.
Retinal Health in High Myopia
Many people who consider ICL surgery have high myopia. High myopia means your eye is longer than average, which can place extra stress on the retina, the light-sensitive layer at the back of your eye. This can sometimes be associated with retinal thinning, lattice degeneration, retinal tears, or other changes.
It is important to understand that ICL surgery does not cause these retinal conditions. Instead, they are related to high myopia itself, which is why careful assessment of the back of your eye is essential before any surgical decision is made.
A complete ICL consultation should always include a thorough retinal examination, not just checks of the front of your eye. This helps ensure that any existing retinal risks are identified early, so your surgeon can plan treatment safely and appropriately for your individual eye health.
Comparing ICL With LASIK in Asian Patients
LASIK and ICL are both effective vision correction options, but they work in different ways. LASIK reshapes the cornea to correct vision, while ICL places a lens inside the eye without permanently altering the corneal structure. Because of this, each procedure has different suitability requirements.
For some Asian patients, LASIK may be completely appropriate and provide excellent results. For others, ICL may be the safer option, particularly if there is a high prescription, thinner corneas, dry eye concerns, or certain anatomical factors that make corneal surgery less suitable.
If you are considering ICL surgery in London, your consultation should clearly explain why it is suitable for your specific eyes. It should not just be presented as an alternative to LASIK, but as a carefully selected option based on detailed measurements and your individual eye health.
Is ICL Riskier in Asian Eyes?
ICL surgery is not automatically riskier in Asian eyes. In fact, many studies from Asian populations show good visual outcomes when patients are carefully selected and the measurements are within safe limits. The key factor is not ethnicity itself, but whether the eye anatomy is suitable for the lens.
The most important part of safety is accurate patient selection and correct lens sizing. If your internal eye measurements are appropriate and the procedure is planned carefully using detailed imaging, ICL can be a very effective vision correction option with strong long-term results.
However, if your anterior chamber is too shallow, vault prediction is uncertain, or the drainage angle is narrow, your surgeon may advise against ICL and recommend an alternative treatment instead. This careful approach is designed to prioritise safety and protect your long-term eye health.
Why Personalised Assessment Matters

Personalised assessment is the most important part of planning ICL surgery. While ethnicity may provide useful background information in research and help guide general understanding of risk patterns, it cannot determine whether you are suitable for treatment or what the safest option is for you as an individual patient. Your eyes still need to be assessed on their own specific features and health status.
Your surgeon will rely on detailed measurements of your eyes, including corneal shape, prescription, anterior chamber depth, white-to-white distance, vault prediction, endothelial cell count, eye pressure, and retinal health. These results give a clear and individual picture of your eye safety and suitability.
This is why two patients from the same ethnic background can receive very different recommendations. Even if you share similar demographics, your measurements and eye anatomy are unique, and they ultimately determine the safest and most effective treatment plan for you.
What Research Means for Patients
Research suggests that ICL surgery can produce good visual outcomes in Asian patients when careful measurements and appropriate patient selection are used. Studies also show that predicting lens vault and choosing the correct lens size remain important parts of achieving safe and effective results.
Newer calculation methods, advanced anterior segment imaging, and AI-based tools may help improve surgical planning and make outcomes more predictable. Some research comparing vault prediction in Asian and White eyes also suggests that biometric differences between populations can influence planning accuracy, which is why precise measurements are so important.
For you as a patient, this means the quality of the clinic matters. The best outcomes are usually seen in centres that take detailed measurements seriously, use modern diagnostic tools, and clearly explain what those measurements mean for your individual surgery.
When ICL May Not Be Suitable
ICL surgery may not be suitable if your eye anatomy is not within safe limits. This includes situations where the anterior chamber is too shallow, the endothelial cell count is too low, the drainage angle is narrow, or your eye pressure is not well controlled. Any significant underlying eye health issues may also make the procedure unsuitable.
It may also not be recommended if your expectations are not realistic or if another treatment option would provide a safer or more appropriate outcome. In these situations, your surgeon should explain the reasons clearly and help you understand the alternatives.
In refractive surgery, a careful decision not to proceed can be just as important as moving forward. Choosing not to perform ICL when it is not suitable helps protect your long-term eye health and ensures that safety always comes first.
Final Checks Before ICL Surgery
Before you undergo ICL surgery, you should expect a detailed assessment to confirm that the procedure is suitable for your eyes. This may include tests such as refraction, corneal scans, anterior segment imaging, endothelial cell count measurements, pupil size assessment, eye pressure checks, and a retinal examination. These investigations help your surgeon plan treatment and identify any factors that may affect safety or outcomes.
You should also have the opportunity to discuss alternative vision correction options and ask questions about the procedure. A thorough consultation should cover the potential benefits, limitations, and whether ICL surgery is the most appropriate choice for your individual needs.
It is equally important that you understand the possible risks, recovery process, follow-up schedule, and long-term monitoring requirements. Although the ICL lens can be removed if necessary, it is still a form of intraocular surgery and should be approached carefully. Good preparation can help reduce avoidable risks, set realistic expectations, and give you greater confidence before treatment.
FAQs:
- Is ICL surgery suitable for Asian eyes?
Yes. ICL surgery can be suitable for many Asian eyes, but suitability is based on individual eye measurements rather than ethnicity. Factors like anterior chamber depth, corneal health, lens position, and retinal safety are more important than background. - Why is ICL surgery often discussed for Asian patients?
ICL is often discussed because many Asian populations have higher rates of myopia and high myopia. In stronger prescriptions, laser surgery may not always be suitable, so ICL can be considered as an alternative that preserves corneal tissue. - Does being Asian affect ICL results?
No. Being Asian does not directly affect surgical outcomes. Results depend on proper patient selection, accurate lens sizing, surgical technique, and healthy eye anatomy. When these are suitable, outcomes are generally very good. - What eye measurements are needed for ICL surgery?
ICL suitability depends on detailed measurements such as anterior chamber depth, white-to-white distance, corneal thickness, endothelial cell count, eye pressure, and retinal health. These help ensure the lens fits safely inside the eye. - What is vault in ICL surgery?
Vault refers to the space between the implanted ICL lens and the natural lens. It is important because too low or too high vault can affect eye pressure or lens safety. Proper planning aims to achieve an ideal, balanced vault. - Is ICL safe for high myopia in Asian patients?
Yes. Research shows that ICL can be safe and effective for high myopia when patients are carefully selected. Many studies in Asian populations report good visual outcomes, but careful screening is essential to minimise risks. - How is ICL different from LASIK?
ICL surgery places a lens inside the eye without removing corneal tissue, while LASIK reshapes the cornea using a laser. ICL is often preferred for thin corneas, very high prescriptions, or patients not suitable for laser surgery. - Can ICL correct astigmatism?
Yes. Toric ICL lenses can correct both myopia and astigmatism together. However, accurate lens alignment is very important, because even small rotation can affect the clarity of vision after surgery. - Who may not be suitable for ICL surgery?
ICL may not be suitable for patients with shallow anterior chamber depth, low endothelial cell count, narrow drainage angles, uncontrolled eye pressure, or certain eye diseases. A full assessment is required to confirm safety. - Does ethnicity affect whether ICL is recommended?
No. Ethnicity does not determine eligibility for ICL surgery. The decision is based entirely on eye anatomy, safety measurements, vision needs, and overall eye health. Ethnicity may only be considered in a research or risk-awareness context.
Final Thoughts: Is ICL Right for Asian Eyes?
ICL surgery can be a highly effective option for many Asian patients, particularly those with moderate to high myopia or thin corneas where laser eye surgery may not be ideal. However, suitability is not determined by ethnicity. Instead, it depends on detailed eye measurements such as anterior chamber depth, endothelial cell health, retinal condition, and overall ocular anatomy. Research shows that when these factors are carefully assessed and the lens is correctly sized, outcomes in Asian patients are generally very good.
The most important takeaway is that ICL is a personalised procedure. Two patients with the same ethnic background can have completely different eligibility based on their eye structure. A thorough assessment ensures safety, accuracy, and long-term stability of results. If you’d like to find out whether ICL surgery in London is suitable for you, feel free to contact us at Eye Clinic London to arrange a consultation.
References:
- Cano‑Ortiz, A., Sánchez‑Ventosa, Á., González‑Cruces, T., Villalva‑González, M., Prados‑Carmona, J.J. and Castillo‑Eslava, R. (2025) Objective rotational analysis of EVO toric ICLs, Journal of Clinical Medicine, 14(9), 2895. Available at: https://www.mdpi.com/2077-0383/14/9/2895
- Kamiya, K., Shimizu, K., Takahashi, M., Ando, W., Hayakawa, H. and Shoji, N. (2021) Eight‑year outcomes of EVO‑ICL implantation in patients with myopia, Frontiers in Medicine. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC8716586/
- Packer, M. (2018) The implantable collamer lens with a central port: review of the literature, Clinical Ophthalmology. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC6267497/
- Al Mahmood, A.S., Reinstein, D.Z., Archer, T.J. and Coleman, D.J. (2014) Risk factors associated with night vision disturbances and refractive changes after phakic intraocular lens implantation, American Journal of Ophthalmology. Available at: https://pubmed.ncbi.nlm.nih.gov/24182745/
- Lee, H., Kang, D.S.Y., Ha, B.J., Choi, J.Y., Kim, E.K. and Seo, K.Y. (2020) Long-term clinical results of posterior chamber phakic intraocular lens implantation to correct myopia, Clinical & Experimental Ophthalmology. Available at: https://pubmed.ncbi.nlm.nih.gov/31981321/