

Angle-Closure vs Open-Angle Glaucoma: Key Differences Explained

The distinction between these forms carries important clinical implications. You may experience slow, silent progression in one type, while the other can develop abruptly with severe symptoms. Urgency and management strategies therefore differ significantly. We tailor care according to the specific pattern identified.
Open-angle glaucoma generally advances gradually and without early warning signs. You might remain unaware of damage until noticeable visual changes occur. Routine screening becomes essential in preventing late diagnosis. We emphasise structured monitoring to detect early structural change.
Angle-closure glaucoma can present far more dramatically. You may develop sudden pain, blurred vision, or nausea that demands urgent attention. Recognising these warning signs allows faster response and safer outcomes. We prioritise clear understanding so you can seek appropriate care without delay.
What Is Glaucoma in General?
Glaucoma describes a group of conditions characterised by optic nerve damage, often associated with raised intraocular pressure. Your optic nerve transmits visual signals from the eye to the brain. When this structure becomes compromised, permanent vision loss can develop. We focus on protecting this vital pathway through early identification.
Intraocular pressure increases when internal fluid fails to drain efficiently. You may not notice any discomfort while sustained pressure gradually injures delicate nerve fibres. Early stages frequently remain symptom-free. We monitor carefully because absence of pain does not indicate absence of harm.
Vision lost to glaucoma cannot be restored. You rely on timely detection to preserve remaining sight. Structured surveillance reduces the risk of silent deterioration. We prioritise proactive management to maintain long-term visual stability.
What Is Open-Angle Glaucoma?
Open-angle glaucoma is the most commonly diagnosed form of the condition. You may not realise that the drainage angle remains physically open in this type. The problem lies in reduced efficiency within the internal outflow system rather than a visible blockage.
- Nature of the Drainage Problem: The angle between the iris and cornea remains structurally open. Fluid exits the eye more slowly due to subtle internal dysfunction.
- Gradual Pressure Increase: Aqueous fluid builds up over time, leading to rising intraocular pressure. This progression is usually painless and develops without obvious warning signs.
- Silent Early Stages: Early glaucoma rarely produces noticeable symptoms.
Routine screening is essential to detect optic nerve damage before vision is affected.
Because changes occur quietly, regular examination becomes your strongest safeguard. We rely on structured testing rather than symptoms alone. Early identification supports timely intervention and long-term visual preservation.
What Is Angle-Closure Glaucoma?
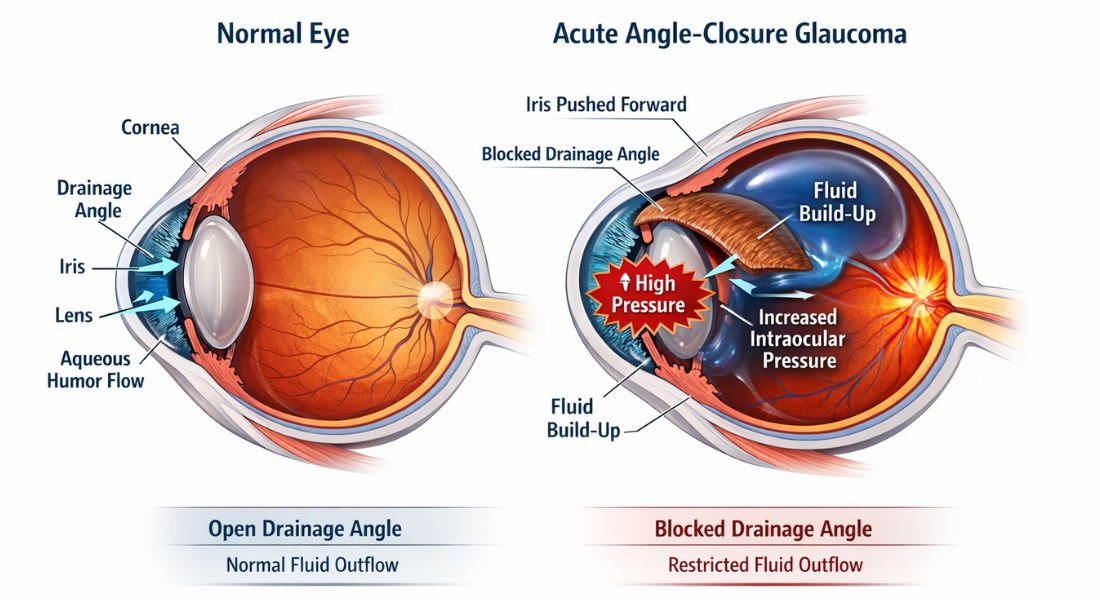
Angle-closure glaucoma develops when your drainage angle becomes obstructed. The iris shifts forward and blocks the normal outflow of aqueous fluid. As a result, intraocular pressure can increase quickly. We recognise this structural blockage as the core mechanism behind the condition.
In some individuals, narrowing progresses slowly and leads to gradual pressure elevation. In others, closure occurs abruptly and triggers severe symptoms. Acute episodes require immediate medical intervention. We treat sudden onset as an ophthalmic emergency.
Your eye’s anatomical configuration plays a decisive role in susceptibility. Naturally narrower angles increase the likelihood of obstruction. Certain structural features place you at higher risk of closure. We evaluate these anatomical factors carefully during examination.
How the Drainage Angle Works
The drainage angle lies at the junction where your cornea meets the iris. Aqueous fluid passes through this space into the trabecular meshwork before leaving the eye. We rely on this pathway to maintain stable intraocular pressure.
In open-angle glaucoma, this channel remains anatomically open but does not function efficiently. You experience gradual pressure build-up due to impaired outflow. In angle closure, the passage becomes physically narrowed or obstructed. We distinguish these mechanisms carefully during assessment.
Variation in structural blockage explains the difference in symptom pattern and urgency. You may notice slow progression in one form and sudden crisis in the other. Recognising the underlying process guides appropriate intervention. We tailor management based on the specific anatomical cause.
Symptoms of Open-Angle Glaucoma

Acute angle closure develops suddenly and with intensity. You may experience severe eye pain, headache, nausea, blurred vision, and coloured halos around lights. The affected eye often becomes visibly red and uncomfortable. We treat this presentation as a medical emergency.
Intraocular pressure can rise sharply within a short period. You face rapid optic nerve damage if intervention is delayed. Visual function can deteriorate quickly without appropriate treatment. We act without hesitation to stabilise the situation.
Urgent care significantly reduces the likelihood of permanent vision loss. You protect your sight by seeking immediate assessment at the first warning signs. Delay increases the risk of irreversible harm. We prioritise swift pressure control to preserve long-term visual health.
Symptoms of Acute Angle-Closure Glaucoma
Acute angle closure develops suddenly and with intensity. You may experience severe eye pain, headache, nausea, blurred vision, and coloured halos around lights. The affected eye often becomes visibly red and uncomfortable. We treat this presentation as a medical emergency.
Intraocular pressure can rise sharply within a short period. You face rapid optic nerve damage if intervention is delayed. Visual function can deteriorate quickly without appropriate treatment. We act without hesitation to stabilise the situation.
Urgent care significantly reduces the likelihood of permanent vision loss. You protect your sight by seeking immediate assessment at the first warning signs. Delay increases the risk of irreversible harm. We prioritise swift pressure control to preserve long-term visual health.
Chronic Angle-Closure Glaucoma
Angle closure is often associated with sudden pain and blurred vision, yet it does not always present in this dramatic way. You may develop gradual narrowing of the drainage angle over time. Understanding this quieter form helps you appreciate the importance of routine review.
- Chronic Angle Narrowing: The drainage angle can become progressively narrower without acute symptoms. Intraocular pressure may rise slowly and without obvious warning signs.
- Subtle or Understated Symptoms: Mild blur or occasional discomfort may occur but can be overlooked. Absence of severe pain does not exclude underlying structural risk.
- Early Detection and Prevention: Regular examinations identify narrowing before complete blockage develops. Preventive laser treatment may be considered to reduce future complications.
Because progression can be silent, structured assessment is essential. We monitor angle anatomy carefully to detect early change. Proactive intervention helps safeguard long-term vision and reduce the risk of sudden pressure spikes.
Risk Factors for Open-Angle Glaucoma
Risk rises noticeably after the age of 40. You face greater susceptibility if close relatives have been affected. High myopia and certain ethnic backgrounds further increase likelihood. We consider these combined factors when assessing overall risk.
Raised intraocular pressure remains one of the strongest contributors. You should recognise, however, that optic nerve damage can still occur even when pressure appears within normal limits. Structural vulnerability varies between individuals. We evaluate the full clinical picture rather than relying on a single reading.
Systemic health also plays an important role in progression. You may experience faster change if conditions such as diabetes or vascular instability are present. Circulatory factors can influence optic nerve resilience. We incorporate wider medical history into long-term management planning.
Risk Factors for Angle-Closure Glaucoma
Angle closure occurs more frequently in individuals with smaller ocular anatomy or shallow anterior chambers. You may carry higher risk if you are long-sighted, as hyperopia often reduces internal space within the eye. Prevalence is also greater in several Asian populations. We assess anatomical structure carefully to identify susceptibility.
Women experience angle closure slightly more often than men. You may develop increased narrowing as the natural lens thickens with age. Progressive crowding within the drainage angle can elevate pressure risk. We monitor these structural changes over time.
Certain medications can precipitate acute closure in predisposed individuals. You should remain cautious if you have known narrow angles before starting new treatments. Prompt evaluation reduces the likelihood of sudden complications. We review medical history thoroughly to minimise preventable triggers.
How Diagnosis Differs
Assessment of both glaucoma types begins with measuring intraocular pressure and examining the optic nerve. You require careful structural evaluation to detect early damage. Distinguishing between forms depends on accurate analysis of the drainage angle. We prioritise detailed examination to guide appropriate management.
Gonioscopy enables direct visual inspection of the angle structures within your eye. You may also undergo imaging such as anterior segment OCT to provide additional anatomical detail. These techniques help clarify whether narrowing or blockage is present. We combine clinical observation with technology for precise diagnosis.
Early recognition of narrow angles allows timely preventative treatment. You reduce the likelihood of acute pressure elevation through proactive intervention. We focus on identifying risk before symptoms emerge.
Treatment of Open-Angle Glaucoma

Open-angle glaucoma is commonly treated initially with prescribed eye drops. You use these to lower intraocular pressure by reducing fluid production or enhancing drainage. Laser procedures may also be introduced as part of a structured management plan.
If pressure remains above target despite medication, surgical options can be discussed. You may benefit from procedures designed to achieve steady and lasting reduction. The objective remains controlled, progressive protection of the optic nerve.
Regular follow-up remains central to effective care. You attend monitoring appointments to track pressure levels and structural change. We ensure ongoing assessment so stability is maintained over time.
Treatment of Angle-Closure Glaucoma
Acute angle closure demands urgent reduction of intraocular pressure. You require rapid-acting medication to stabilise the eye and relieve strain. We act swiftly to prevent permanent optic nerve damage.
Laser peripheral iridotomy forms a tiny opening in the iris to re-establish fluid drainage. You benefit from restored aqueous flow and reduced pressure build-up. We use this procedure to address the underlying anatomical blockage.
In long-standing narrow angles, preventive laser treatment may be recommended before any acute episode develops. You lower your risk through early intervention and structured follow-up. We prioritise timely management to safeguard visual function.
Why Urgency Differs
Open-angle glaucoma typically advances at a gradual pace. You are able to follow a structured treatment plan with adjustments made over time. We monitor progression carefully to maintain stability and protect vision.
Angle-closure glaucoma, especially in its acute form, requires urgent medical intervention. You may experience sudden pain, blurred vision, or halos around lights. We treat these symptoms as emergencies to prevent permanent damage.
Awareness of warning signs allows quicker and more appropriate action. You reduce the risk of vision loss by responding promptly to abrupt changes. We emphasise clear distinction between these forms to avoid harmful delay.
Can One Type Turn Into the Other?
Open-angle and angle-closure glaucoma are distinct conditions with different underlying mechanisms. You may appear to have open angles initially, even if subtle narrowing is developing. Careful examination helps identify early anatomical changes before complications arise.
- Different Mechanisms of Disease: Open-angle and angle-closure glaucoma involve separate structural processes. Gradual narrowing can sometimes precede later angle closure.
- Age-Related Anatomical Change: Advancing age may increase crowding within the drainage angle. These shifts can raise the likelihood of pressure elevation over time.
- Importance of Early Recognition: Timely detection allows preventive or therapeutic intervention. Structured follow-up reduces the risk of sudden pressure spikes.
By monitoring angle anatomy over time, we identify subtle transitions before they become urgent. You benefit from proactive management tailored to structural findings. Consistent surveillance supports long-term visual stability and protection.
Importance of Screening
Open-angle glaucoma develops without noticeable symptoms, which makes routine screening crucial. You cannot rely on pressure measurements alone to exclude disease. Comprehensive assessment includes optic nerve imaging and detailed visual field analysis. We use this combined approach to detect subtle early change.
If you carry recognised risk factors, consistent eye examinations become even more important. You improve your chances of preserving sight through timely identification of progression. Regular monitoring allows small shifts to be addressed before significant damage occurs. We emphasise prevention rather than reaction.
A structured approach to glaucoma treatment in London prioritises individual risk profiling and ongoing surveillance. You receive tailored monitoring schedules based on your clinical findings. Early intervention strategies are introduced where necessary to protect visual function. We focus on maintaining long-term stability through personalised care.
FAQs:
- How can you tell whether you have open-angle or angle-closure glaucoma?
You cannot determine the type based on symptoms alone in most cases. We examine the drainage angle directly using specialised assessment techniques. Accurate classification depends on anatomical evaluation rather than guesswork. - Why does open-angle glaucoma often go unnoticed for years?
You may not experience discomfort or obvious vision change in early stages. We find that damage develops quietly in peripheral vision before affecting central sight. Regular testing is therefore essential for early detection. - What warning signs should prompt you to seek urgent help?
You should act immediately if you develop sudden eye pain, blurred vision, headache, or nausea. We treat abrupt pressure elevation as an emergency requiring rapid intervention. Early response significantly reduces the risk of permanent harm. - Are both types linked to high eye pressure?
You often see raised pressure in both forms, but the mechanism differs. We recognise that blockage causes rapid elevation in angle closure, whereas gradual outflow resistance drives open-angle disease. Structural differences determine the pattern. - Can you have narrow angles without symptoms?
Yes, you may have narrowing without noticeable discomfort. We frequently detect this during routine examination before any acute event occurs. Preventive treatment can then reduce the risk of sudden closure. - Does treatment differ between the two forms?
You usually manage open-angle glaucoma with long-term pressure-lowering therapy. We often use laser procedures in angle closure to relieve anatomical obstruction. The strategy reflects the underlying mechanism rather than a single approach. - Are certain people more at risk of angle closure?
You may face higher risk if you are long-sighted or have smaller ocular anatomy. We also observe increased likelihood in specific ethnic backgrounds and with advancing age. Structural crowding plays a key role. - Can open-angle glaucoma suddenly become an emergency?
Open-angle disease generally progresses gradually rather than abruptly. We monitor carefully because changes occur over time rather than in hours. Sudden severe symptoms are more typical of acute angle closure. - Why is screening important even if your vision feels normal?
You may retain clear central vision despite ongoing peripheral loss. We rely on imaging and visual field testing to identify early damage. Waiting for symptoms can delay timely protection. - Can both forms be controlled with early diagnosis?
Yes, you greatly improve long-term outlook when the condition is identified promptly. We tailor intervention according to the specific type and severity. Structured follow-up remains essential to preserve stable vision over time.
Final Thought: Angle-Closure vs Open-Angle Glaucoma
Open-angle and angle-closure glaucoma differ significantly in mechanism, symptoms, and urgency. Open-angle glaucoma develops slowly and silently, while angle-closure glaucoma can present suddenly with severe pain and rapid pressure rise. Recognising these differences supports timely diagnosis and appropriate management. Early detection remains central to preserving vision in both forms.
The situation is addressed through accurate angle assessment, regular monitoring, and tailored glaucoma treatment based on your individual risk and disease type. If you are concerned whether glaucoma treatment in London could benefit you, feel free to get in touch with us at Eye Clinic London.
References:
- Potop, V., Dragosloveanu, C.D.M., Ciocâlteu, A.M., et al., 2024. The Mirror Theory: Parallels between open angle and angle closure glaucoma. Life (Basel), 14(9), 1154. https://pubmed.ncbi.nlm.nih.gov/39337937/
- Wang, C., Chen, D.-F., Shang, X., et al., 2024. Evaluating Diagnostic Concordance in Primary Open‑Angle Glaucoma Among Academic Glaucoma Subspecialists. Diagnostics, 14(21), 2460. https://www.mdpi.com/2075-4418/14/21/2460
- Wang, Y., Guo, Y., Zhang, Y., et al., 2024. Differences and Similarities Between Primary Open Angle Glaucoma and Primary Angle‑Closure Glaucoma. Eye and Brain, 16, pp.39–54. https://pubmed.ncbi.nlm.nih.gov/39309574/
- Wagner, I.V., 2022. Updates on the Diagnosis and Management of Glaucoma. https://www.sciencedirect.com/science/article/pii/S2542454822000686
- Sun, X., Dai, Y., Chen, Y., et al., 2017. Primary angle‑closure glaucoma: What we know and what we don’t know. https://www.sciencedirect.com/science/article/pii/S1350946216300519