

Blocked Tear Duct Surgery in Children: When Is It Needed?
")
Your child’s eyes naturally produce tears throughout the day to keep the surface moist and protected. These tears usually drain through tiny openings in the inner corner of the eyelids and into the nose. When this drainage pathway is blocked, tears spill over onto the cheek instead of draining properly. You might notice constant watering even when your child is not crying.
In newborns, the tear duct system may not yet be fully developed. A thin membrane can remain over the nasal opening of the duct, preventing normal tear drainage. This is the most common reason babies experience persistently watery eyes. You may also see mild stickiness or crusting around the lashes, especially after sleep.
Although it can look worrying, this condition is usually harmless in early infancy. In most cases, the tear duct opens naturally within the first year of life. You are often advised to gently massage the area and keep the eye clean while waiting for improvement. Careful monitoring is typically all that is needed at this stage.
Why Blocked Tear Ducts Are So Common in Babies
Blocked tear ducts affect many newborns and young infants, so you are not alone if you notice this in your baby. The condition is surprisingly common and, in most cases, temporary. The main reason is that your baby’s tear drainage system is still developing. Immature tear ducts simply do not drain tears as efficiently as they will later on.
At birth, the lower end of the tear duct may still be sealed by a thin membrane. As your baby grows, this membrane usually opens on its own. Natural developmental changes allow the drainage pathway to function properly. In most children, this simple maturation process solves the issue without any intervention.
Because spontaneous resolution is so common, surgery is rarely recommended straight away. You will usually be advised to follow a conservative approach first, which may include gentle massage and keeping the eye clean. Regular monitoring helps ensure there are no signs of infection. In many cases, time alone allows the blockage to clear naturally.
Typical Symptoms Parents Notice
The most common sign you will notice is constant watering from one or both of your child’s eyes. Tears may pool along the lower eyelid and spill onto the cheek even when your child is calm. You might also see a sticky discharge collecting in the corners of the eye. The eyelids can look slightly crusted, particularly after sleep.
Importantly, the white part of your child’s eye usually remains clear and bright. Significant redness, swelling or obvious discomfort is not typical with a simple blocked tear duct. If you do notice redness or your child seems unusually unsettled, an infection may be developing. In that case, you should seek medical advice promptly.
You may find that symptoms become more noticeable in cold weather or when your child has a mild cold. Nasal congestion can temporarily increase tearing because the drainage system connects to the nose. This can make the watering seem worse for a short time. However, it does not necessarily mean the condition has permanently worsened.
When Massage Is Recommended
Tear duct massage is often recommended to help encourage the duct to open naturally. By applying gentle pressure to the inner corner of your child’s eye, you may help move trapped fluid through the drainage channel. Your clinician will usually show you the correct technique so you feel confident doing it at home. When performed properly, it is safe and simple to include in your daily routine.
You are typically advised to carry out the massage several times a day. Consistency matters, as regular gentle pressure can improve the chances of the membrane opening on its own. Many parents begin to notice gradual improvement over a number of weeks. The watering may slowly reduce, and discharge can become less frequent.
However, massage does not guarantee that the blockage will resolve. If symptoms continue beyond the first year of life, further assessment may be needed. Your clinician will review your child’s progress and discuss whether additional treatment should be considered. Regular follow-up helps ensure the right decision is made at the right time.
When Natural Resolution Becomes Less Likely
If your child’s tearing continues beyond 12 months of age, natural resolution becomes less likely. By this stage, the membrane at the end of the tear duct would usually have opened on its own. Persistent watering suggests that the blockage may not clear without help. At this point, further evaluation becomes more important.
Ongoing tearing can start to affect your child’s comfort and day-to-day hygiene. You may find yourself constantly wiping the eyes, and recurrent sticky discharge can become frustrating for both you and your child. Although the condition is rarely dangerous, delaying treatment can unnecessarily prolong these symptoms. Over time, repeated infections may also become more likely.
An assessment at this stage helps determine whether a simple procedure, such as probing, is appropriate. Early intervention generally improves success rates and reduces the chance of ongoing problems. A timely review allows you to make an informed decision about the next step. Acting at the right moment often leads to quicker, smoother resolution.
Recurrent Infections as a Warning Sign
If your child keeps developing conjunctivitis linked to poor tear drainage, it may signal that further treatment is needed. When tears cannot drain properly, they stagnate. This creates an environment where bacteria can grow more easily.
- Blocked tear ducts increase infection risk: Stagnant tears allow bacteria to multiply, leading to repeated episodes of sticky discharge and redness. These infections can become frustratingly frequent.
- Repeated antibiotics are not a long-term solution: While antibiotic drops may clear each episode temporarily, they do not correct the underlying blockage. Addressing the obstruction treats the root cause rather than just the symptoms.
- Surgical probing can prevent further infections: A simple probing procedure is often effective in opening the duct. Once drainage improves, infections usually reduce significantly.
If you notice swelling near the inner corner of the eye, seek urgent medical advice. This could indicate dacryocystitis, a more serious infection of the tear sac. Prompt treatment reduces the risk of complications. Early intervention helps restore comfortable, healthy tear drainage.
What Is Tear Duct Probing?
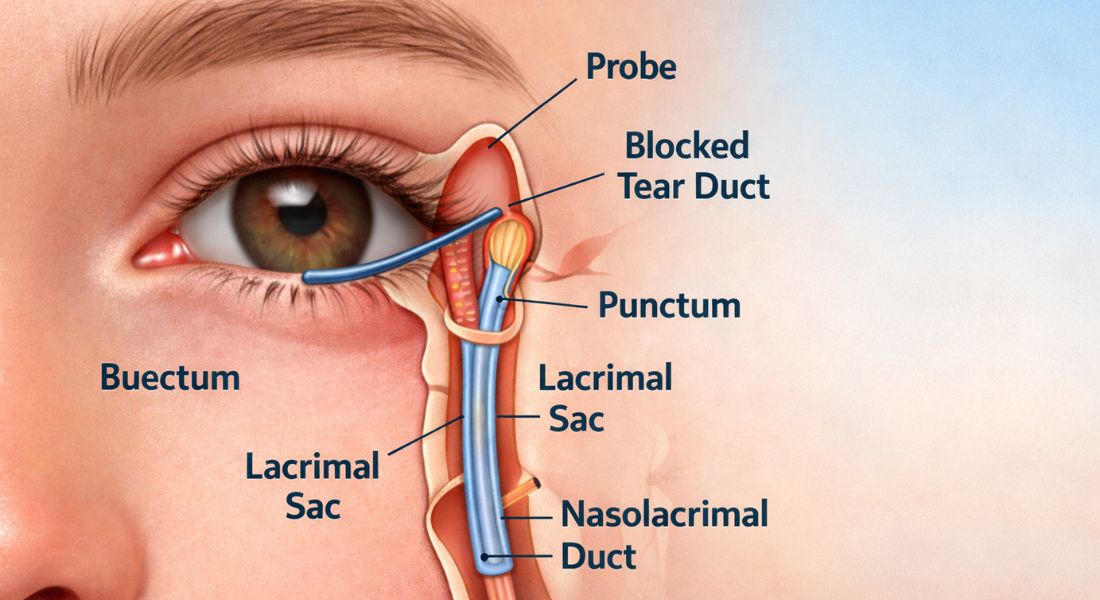
Tear duct probing is a minor surgical procedure used to open a blocked tear drainage pathway. During the procedure, a very fine instrument is gently passed through your child’s natural tear opening in the eyelid. This allows the clinician to clear the obstruction from within the duct. No external cuts are made, as the natural drainage channel is used.
In young children, the procedure is usually carried out under a short general anaesthetic. This ensures your child remains completely still and comfortable throughout. The process itself typically takes only a few minutes to complete. In most cases, you and your child can return home the same day.
Afterward, there are no visible stitches or scars because the technique does not involve external incisions. The body’s own drainage route is simply opened to restore normal tear flow. This approach makes probing minimally invasive. It is also highly effective, particularly when performed at the right time.
Why General Anaesthetic Is Used
If your child requires a tear duct procedure, you may wonder why a general anaesthetic is recommended. The reason is simple: young children cannot reliably stay still during delicate surgery around the eye. Even small movements could increase the risk of injury.
- Stillness ensures safety and precision: Procedures near the eye require extremely fine instruments and careful control. A brief general anaesthetic allows the surgeon to work safely and accurately.
- Modern paediatric anaesthesia is closely monitored: Specialist paediatric anaesthetists carefully control and supervise your child throughout the procedure. Monitoring equipment tracks breathing, heart rate, and oxygen levels continuously.
- Recovery is usually quick: Most children wake comfortably within a short time. In many cases, you can take your child home the same day.
Anaesthetic risk is very low in otherwise healthy children. A pre-operative assessment ensures your child is suitable for treatment. Strict safety protocols are followed at every stage. The goal is always to provide effective care in the safest possible way.
Success Rates of Probing
Probing has excellent success rates, particularly if your child is under two years old. Most children experience a noticeable reduction in watering soon after the procedure. In many cases, you may see improvement within just a few days. The constant overflow of tears often settles quickly once the blockage is cleared.
Success rates are generally above 80–90 per cent in younger children. While outcomes can be slightly lower in older children, they are still very favourable overall. Acting earlier tends to improve the likelihood of complete resolution. This is why timely assessment and treatment planning are important.
If the blockage does not fully resolve, a repeat procedure may be considered. In some cases, additional techniques such as silicone tube insertion are used to keep the duct open for longer. The right approach depends on how your child responds after the initial treatment. Careful follow-up helps guide the next step if needed.
What Happens After Surgery

After your child’s procedure, you may notice some mild redness or watering. This is common and usually settles within a few days. Recovery is generally straightforward and well tolerated.
- Mild irritation is normal: Slight redness, watering, or minimal discharge can occur temporarily. These symptoms typically improve quickly as the eye heals.
- Antibiotic drops are often prescribed: You may be given drops to use for a short period to reduce the risk of infection. Following the instructions carefully supports smooth healing.
- Return to normal activities is usually rapid: Most children resume their usual routine within 24 hours. There are rarely significant restrictions after simple tear duct procedures.
Follow-up appointments help confirm that tear drainage has improved. These visits are typically brief and reassuring. Ongoing problems are uncommon after successful treatment. With proper care, most children recover quickly and comfortably.
Risks and Complications
Tear duct probing is considered a very safe procedure for your child. Minor bleeding or temporary irritation can occasionally occur, but these usually settle quickly without lasting effects. Your child’s eye may look slightly watery or mildly red for a short time. Serious complications are extremely rare.
In very uncommon cases, the tear duct can become blocked again after the procedure. If this happens, further treatment may be discussed to restore proper drainage. Careful follow-up appointments help detect any early signs of recurrence. Prompt review reduces the likelihood of prolonged symptoms.
Overall, when surgery is timed appropriately, the benefits clearly outweigh the risks. An experienced surgical team and careful technique further enhance safety and success. You should also feel reassured that this is a well-established and commonly performed procedure. Clear communication and guidance are an important part of your child’s care.
Alternative Treatments If Probing Fails
If simple probing does not fully resolve your child’s blocked tear duct, there are still effective options available. While this situation is uncommon, it can be managed safely with additional treatment. Your specialist will guide you through the next steps if needed.
- Silicone stenting may be recommended: A tiny silicone tube can be placed inside the tear duct to keep it open during healing. This provides longer-term support and is usually temporary.
- Balloon dilation is sometimes considered: A small balloon device can be used to gently widen the duct. This technique helps improve drainage in selected cases.
- More complex surgery is rarely required: Advanced procedures are reserved for persistent or unusual cases. These are uncommon and carefully planned by specialists.
The vast majority of children respond well to initial probing. Additional procedures are only needed in a small percentage of cases. Careful specialist assessment ensures the most appropriate approach. With structured management, long-term outcomes are typically excellent.
Emotional Reassurance for Parents
It is completely normal for you to feel anxious when surgery is mentioned. Even a minor procedure can feel overwhelming when it involves your child. You may worry about anaesthetic, recovery, or possible complications. Clear explanations and honest discussions can significantly reduce that fear.
Blocked tear duct surgery is one of the most straightforward paediatric eye procedures performed today. It is quick, safe and highly effective in the majority of cases. The anaesthetic is short, and recovery is usually smooth. Knowing these facts often helps you feel more reassured and in control.
Open communication with your specialist plays an important role in building your confidence. You should feel comfortable asking any questions, no matter how small they seem. Understanding each step of the process helps you prepare mentally and practically. When you are well informed, you naturally feel calmer and better equipped to support your child.
Long-Term Outlook
The long-term outlook after successful tear duct probing is excellent. Most children experience complete resolution of watering and discharge. Once the blockage is cleared, symptoms usually settle fully. There are typically no lasting effects on the eye or surrounding structures.
Normal tear drainage continues without further difficulty. When managed at the right time, your child’s visual development is not affected. Early and appropriate treatment helps protect both comfort and overall eye health. In most cases, life simply returns to normal without ongoing concerns.
Once the issue has resolved, recurrence is uncommon. Follow-up appointments provide reassurance that healing has progressed as expected. You can feel confident that the vast majority of children go on to have no future problems. The outcome is overwhelmingly positive.
When to Seek Specialist Review

If your child’s watering continues beyond one year of age, you should seek specialist advice. Recurrent infections, swelling near the inner corner of the eye, or increasing discharge also warrant prompt evaluation. Early review helps ensure that any necessary treatment is not delayed. Acting at the right time can prevent ongoing discomfort.
Consulting an experienced paediatric ophthalmologist in London can give you clarity and reassurance. A thorough examination will confirm whether simple monitoring is still appropriate or if a procedure such as probing is needed. Clear professional guidance allows you to understand the options fully. This helps you make decisions with confidence rather than uncertainty.
Delaying assessment can unnecessarily prolong symptoms and frustration. Early specialist input often simplifies care and improves success rates. When you seek expert evaluation promptly, you give your child the best chance of quick and effective resolution. Timely action truly makes a difference.
Difference Between Simple and Complex Obstruction
Most blocked tear ducts in children are caused by a simple membrane obstruction at the lower end of the duct. This thin membrane prevents tears from draining properly but is usually straightforward to treat. In these cases, probing is highly effective and often resolves the problem quickly. The majority of children fall into this simple category.
More complex obstructions are less common but can occur. These may involve structural narrowing of the duct or abnormalities along the drainage pathway. In such situations, additional techniques beyond standard probing may be required. This could include silicone tube insertion or other specialised approaches.
Understanding the exact type of blockage is essential for proper treatment planning. A careful specialist examination helps identify whether the obstruction is simple or complex. Accurate diagnosis increases the likelihood of success. When care is tailored to your child’s specific condition, outcomes are generally excellent.
Impact on Vision
Blocked tear ducts usually do not directly affect your child’s vision. The problem relates to tear drainage rather than the structures responsible for sight. In most cases, visual development progresses normally despite the watering. However, if repeated infections are left untreated, they could potentially cause temporary discomfort that interferes with normal visual behaviour.
Prompt management helps prevent these secondary complications. When tear drainage is restored, the surface of the eye remains clearer and healthier. Maintaining comfort encourages your child to open their eyes normally and engage visually with their surroundings. This supports healthy visual development during important early stages.
Regular paediatric eye reviews provide reassurance that everything remains on track. This is particularly important in infancy and early childhood, when vision is still developing rapidly. Ongoing monitoring allows any concerns to be addressed early. Protecting tear drainage and eye health ultimately protects long-term vision.
Hygiene and Home Care Before Surgery
Before surgery is considered, simple home care plays an important role in managing your child’s symptoms. Keeping the eye clean can reduce irritation and discomfort. Conservative treatment is always the first step in infancy.
- Gently clean away discharge: You can wipe away sticky discharge using sterile cotton wool soaked in cooled, boiled water. Always wipe from the inner corner outward and use a fresh piece each time.
- Wash your hands before and after care: Clean hands reduce the risk of introducing further bacteria. Good hygiene makes a meaningful difference.
- Avoid unprescribed medications: Antibiotic drops should only be used if your doctor advises them. Overuse can contribute to resistance and is not helpful without clear infection.
Simple hygiene measures often keep symptoms manageable while natural drainage improves. Many blocked tear ducts resolve without surgery. Careful observation helps determine whether further treatment is truly necessary. Surgery is considered only when conservative care has not been sufficient.
Timing Matters
When it comes to tear duct surgery, timing is carefully considered. Many blocked ducts resolve naturally during the first year of life. The decision to intervene balances patience with persistent symptoms.
- Waiting allows for natural resolution: In many infants, tear drainage improves on its own. Acting too early may expose your child to a procedure that ultimately was not necessary.
- Delaying too long can prolong discomfort: Ongoing watering, discharge, or repeated infections can affect comfort and daily care. Persistent symptoms may justify earlier intervention.
- Specialist review usually occurs around 9–12 months: If symptoms continue beyond this stage, your specialist will reassess. Individual factors always influence the final decision.
Choosing the right time maximises the likelihood of success. Younger children generally respond very well to probing procedures. Careful, personalised assessment guides safe decision-making. Well-timed intervention supports smooth recovery and long-term comfort.
Frequently Asked Questions:
- How do you know if your child really needs blocked tear duct surgery?
You may be advised to consider surgery if your child’s watering persists beyond 12 months of age, especially if massage has not worked. Recurrent infections, repeated antibiotic use, or swelling near the inner corner of the eye are also important signs. A specialist examination confirms whether the blockage is likely to resolve on its own or whether probing would provide a more permanent solution. - Is blocked tear duct surgery painful for your child?
The procedure itself is not painful because it is performed under a short general anaesthetic. Your child will be asleep throughout and will not feel anything during the probing. Afterwards, there may be mild irritation or watering, but this usually settles quickly and does not cause significant discomfort. - How long does the tear duct probing procedure take?
The actual probing procedure usually takes only a few minutes. However, you should expect to be at the hospital longer due to admission checks, anaesthetic preparation, and recovery time. In most cases, you are able to take your child home on the same day. - Is general anaesthetic safe for young children?
Modern paediatric anaesthesia is very carefully controlled and monitored by experienced specialists. In otherwise healthy children, the risk is extremely low. Your child will have a pre-operative assessment to ensure they are suitable for anaesthesia, which adds an additional layer of safety. - What if the tear duct becomes blocked again after surgery?
In a small number of cases, the duct can re-block. If this happens, your specialist may recommend a repeat probing or consider inserting a small silicone tube to keep the duct open during healing. The vast majority of children respond well to the first procedure and do not require further intervention. - Will surgery affect your child’s vision development?
Blocked tear ducts themselves do not usually affect vision because the issue involves drainage rather than the visual structures of the eye. When treated appropriately, tear duct surgery does not interfere with visual development. Prompt management also reduces the risk of infection, which helps protect long-term eye health. - Can you avoid surgery if you wait longer?
In younger infants, waiting is often appropriate because many cases resolve naturally. However, if symptoms continue beyond one year of age, spontaneous resolution becomes less likely. Waiting too long may prolong discomfort and repeated infections, so timing should be guided by specialist advice. - What should you expect after your child comes home?
You may notice mild redness or slight watering for a few days. Antibiotic drops are commonly prescribed, and you will be given instructions on how to use them. Most children return to their usual activities within 24 hours, and recovery is generally smooth. - Are there alternatives if simple probing does not work?
If initial probing is unsuccessful, additional techniques such as silicone stenting or balloon dilation may be considered. These approaches are typically reserved for more persistent or complex cases. Your specialist will explain the most suitable option based on your child’s individual condition. - When should you seek urgent medical attention?
You should seek urgent review if you notice swelling, redness, or tenderness near the inner corner of the eye, particularly if your child seems unwell. This may indicate an infection of the tear sac that requires prompt treatment. Early assessment ensures complications are avoided and appropriate care is given quickly.
Final Thought: When to Consider Specialist Care for Your Child
If your child has a blocked tear duct, it is completely natural for you to feel concerned. The constant watering, sticky discharge, and occasional infections can be frustrating and worrying. However, in most cases, the condition improves naturally during the first year of life with simple measures such as massage and careful hygiene.
When symptoms persist beyond infancy or infections become recurrent, timely intervention can make a significant difference. Tear duct probing is a quick, safe, and highly effective procedure when performed at the right time. With appropriate assessment and expert care, the long-term outlook for your child is excellent. If you’d like to find out whether paediatric ophthalmologist in London is suitable for you, feel free to contact us at Eye Clinic London to arrange a consultation.
References:
- Blazon, M.N., Rezar‑Dreindl, S., Wassermann, L. and Neumayer, T., 2024. Retinopathy of Prematurity: Incidence, Risk Factors, and Treatment Outcomes in a Tertiary Care Center. Journal of Clinical Medicine, https://www.mdpi.com/2077-0383/13/22/6926
- Albanese, G.M., Visioli, G., Alisi, L., Armentano, M., Giovannetti, F., Lucchino, L., Marenco, M., Pontecorvi, P. and Gharbiya, M., 2025. Retinopathy of Prematurity and MicroRNAs. Biomedicines. https://www.mdpi.com/2227-9059/13/2/400
- Fevereiro‑Martins, M., Marques‑Neves, C., Guimarães, H. and Bicho, M., 2023. Retinopathy of Prematurity: A Review of Pathophysiology and Signalling Pathways. Survey of Ophthalmology, https://pubmed.ncbi.nlm.nih.gov/36427559/
- Strelnikov, J.I., Rao, R., Majidi, S., Lueder, G. and Reynolds, M.M., 2024. Retinopathy of Prematurity Screening: Prevalence and Risk Factors of Ophthalmic Complications in Non‑Treated Preterm Infants. https://pubmed.ncbi.nlm.nih.gov/38212403/
- Chan‑Ling, T., 2018. Pathophysiology, Screening and Treatment of Retinopathy of Prematurity: A Multi‑Disciplinary Perspective. Progress in Retinal and Eye Research, https://www.sciencedirect.com/science/article/abs/pii/S1350946216300775